

ECMO-treated respiratory failure and asthma exacerbations reduce mortality 2023
Zakrajsek and colleagues examined 13,714 patients with refractory AERF in ECMO-capable institutions from 2010 to 2020 to see if ECMO reduces mortality.
According to researchers, asthma exacerbation patients required to be hospitalized and treated with short-acting bronchodilators, systemic corticosteroids, and invasive ventilation.
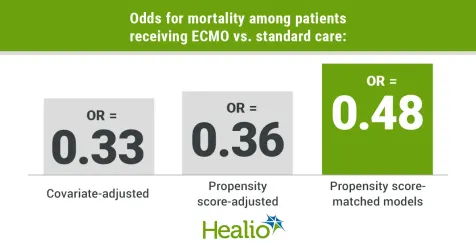
In covariate-adjusted, propensity score-adjusted, and propensity score-matched models, researchers compared hospital mortality chances for ECMO and standard care patients.
Researchers examined mortality, ICU length of stay, hospital length of stay, invasive ventilation time, hospital expenses, and safety outcomes compared the two therapy groups.
127 individuals (mean age, 38 years; 54.3% women) underwent ECMO, while 13,587 (mean age, 46 years; 64.2% women) did not. Most ECMO patients got venovenous (n = 105) rather than venoarterial (n = 8) or a combination of both (n = 14). After admission, ECMO started on day 2.5 (range, 1-19 days) and lasted 4 days (range, 1-49 days).
Mortality
1,540 (11.2%) research subjects died.
In all three models, ECMO recipients had lower mortality odds than those receiving standard care: covariate-adjusted (OR = 0.33; 95% CI, 0.17-0.64), propensity score-adjusted (OR = 0.36; 95%, 0.16-0.81), and propensity score-matched (OR = 0.48; 95%, 0.24-0.98).
In a sensitivity study of individuals treated with ECMO within 7 days of hospitalization (n = 120), only the covariate-adjusted model showed lower death risks (OR = 0.48; 95% CI, 0.23-0.98).
In two models, ECMO reduced death in patients from 499 ECMO-capable hospitals and 377 hospitals without ECMO (covariate-adjusted model, OR = 0.35; 95% CI, 0.19-0.67; propensity score-adjusted model, OR = 0.39; 95%, 0.18-0.87).
Adverse incidents,
ECMO did not reduce ICU, hospital, or invasive ventilation stays. However, co-variate-adjusted (1.5; 95% CI, 1.31-1.71), propensity score-adjusted (1.79; 95%, 1.49-2.14), and propensity score-matched models (1.59; 95%, 1.32-1.91) models demonstrated a substantial increase in mean hospital expenditures with ECMO. According to the propensity score-matched model, each patient treated with ECMO cost $113,789 (95% CI, $65,968-$161,611; P <.0001).
In the propensity score matched sample of 82 ECMO patients and 164 non-ECMO patients, researchers found just two notable variations in adverse events. ECMO patients had higher hemorrhage (9 vs. 2), but non-ECMO patients had more brain death (8 vs 0).
Importantly, Zakrajsek and colleagues warn that their findings need confirmation in other investigations.
“We wish to emphasize that although this is the largest controlled study to address the impact of ECMO for people with AERF, the results may still be subject to bias […], and therefore should only be considered hypothesis generating,” Zakrajsek and colleagues noted. “ECMO efficacy for AERF requiring mechanical ventilation must be determined by a randomized clinical trial. Naturally, any clinical trial would optimize standard and supplementary AERF therapy, including permissive hypercapnia, before enrollment.
This study by Zakrajsek and colleagues provides a start to understanding ECMO treatment in AERF patients, but as the researchers suggest, more information needs to be captured on the specific patients who may benefit from this option, according to an accompanying editorial by Orlando Garner, MD, intensivist at Midland Memorial Hospital, and Nicola A. Hanania, MD, FCCP, professor in the section of pulmonary and critical care medicine at Baylor College of Medicine.
“Patients with life-threatening asthma exacerbations [LTAE] who required mechanical ventilation were identified using ICD-9 and ICD-10 codes,” Garner and Hanania reported. This study rarely used ECMO, and the selection of individuals for cannulation is uncertain. This is crucial if such a method is to be widely used in LTAE patients. High-risk ventilator-induced lung damage patients and those with refractory hypoxemia and hypercarbia confined by high ventilatory pressures may benefit from such an intervention.


